
Meniscal Injuries

What is the meniscus?
The meniscus is a C-shaped piece of cartilage inside the knee joint. Each knee has two menisci:
- Medial meniscus – on the inner side of the knee
- Lateral meniscus – on the outer side of the knee
The menisci act as:
- Shock absorbers
- Load distributors
- Stabilising structures
- Protectors of the joint surface
A tear in the meniscus is one of the most common knee injuries and can occur at any age.
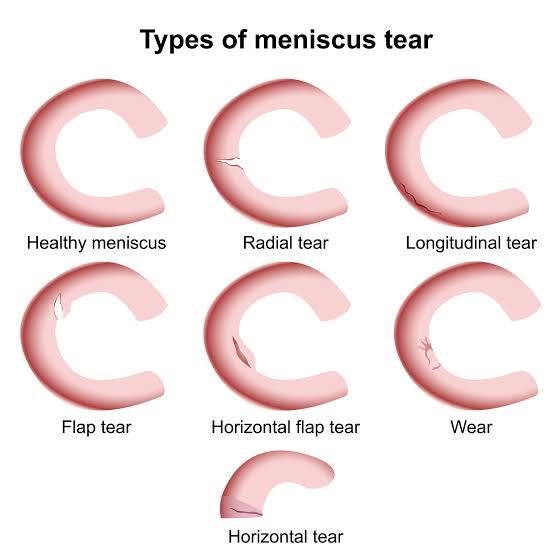
Types of Meniscal Tears
Meniscal tears are broadly divided based on how and why they occur.
→ Twisting movements
→ Pivoting while the foot is planted
→ Sports such as football, rugby, skiing or basketball
These tears are often sudden and may be associated with swelling or a “pop”.
Common Symptoms
Meniscal tears can cause:
- Pain on either the inner or outer side of the knee
- Swelling (sometimes delayed by several hours)
- Clicking, catching or popping
- Locking – inability to fully straighten the knee
- Stiffness or reduced movement
- Giving way or instability
- Pain when twisting, squatting or climbing stairs
- Pain when twisting, squatting or climbing stairs
- Symptoms vary greatly depending on the type, size and location of the tear.
Causes of Meniscal Tears
- Sudden twisting injuries
- Squatting or lifting heavy objects
- Sports with pivoting movements
- Age-related changes
- Joint malalignment
- Coexisting knee arthritis
- Sometimes there is no identifiable cause.
How is a meniscal injury diagnosed?
→ How the injury happened
→ Location of pain
→ Activities that worsen or improve symptoms
→ Any locking, catching or instability
→ Tenderness along the joint line
→ Swelling or fluid in the knee
→ Range of motion
→ Meniscal special tests
→ Ligament stability
→ X-rays help rule out arthritis and bony causes of pain
→ MRI scan is the gold standard for diagnosing a meniscal tear
After this, we will discuss whether your tear is likely to heal, improve with physiotherapy or require surgery.
01
Patient History
We will discuss:
- How the injury happened
- Location of pain
- Activities that worsen or improve symptoms
- Any locking, catching or instability
02
Examination
I will assess:
- Tenderness along the joint line
- Swelling or fluid in the knee
- Range of motion
- Meniscal special tests
- Ligament stability
03
Imaging
- X-rays help rule out arthritis and bony causes of pain
- MRI scan is the gold standard for diagnosing a meniscal tear
After this, we will discuss whether your tear is likely to heal, improve with physiotherapy or require surgery.
Non-Surgical Treatment Options
Many meniscal tears—especially degenerative ones—do not require surgery. Non-operative management can be very effective.
Rest and Activity Modification
Avoid deep squatting, twisting or high-impact activity while symptoms settle.
Weight management
A structured programme focuses on:
→ Strengthening the quadriceps, hamstrings and gluteal muscles
→ Improving balance and knee stability
→ Restoring normal movement patterns
Ice and Anti-inflammatory Measures
Useful in early stages or during flare-ups.
Pain Relief
→ Paracetamol
→ NSAIDs (if appropriate)
→ Topical anti-inflammatory gels
Injections
Steroid injections can help reduce inflammation in selected cases, particularly if there is an associated flare of arthritis.
When is surgery recommended?
Surgery may be considered if:
- Symptoms persist despite physiotherapy
- There is mechanical locking
- A large or displaced tear is blocking movement
- Pain significantly affects daily activities or sport
- MRI shows a tear unlikely to heal on its own
- The tear is traumatic in a younger or active patient
Surgery is usually performed arthroscopically (keyhole surgery).
Surgical Options
01
Meniscal Repair
- In suitable tears—especially in younger patients—repairing the meniscus allows it to heal and preserves long-term knee health.
- Advantages
- Preserves natural meniscus
- Helps protect against arthritis
- Suitable for tears in the “red-red” or “red-white” vascular zones
02
Partial Meniscectomy
- If the tear cannot be repaired, the damaged part of the meniscus is trimmed and smoothed.
- Advantages
- Quick recovery
- Improvement in mechanical symptoms (catching, locking)
- Considerations:
- Removing tissue may increase the risk of osteoarthritis over time
- We always aim to preserve as much meniscus as possible
Recovery and Rehabilitation
Recovery depends on the type of treatment:
If treated non-surgically:
- Most patients recover over 6–12 weeks
- Physiotherapy and maintaining strength are key
After meniscal repair:
- Recovery may take 3–4 months
- A brace or limited weight-bearing may be needed
- Physiotherapy is essential to protect the repair
After partial meniscectomy:
- Many patients walk normally within a few days
- Full recovery typically within 4–6 weeks
- Gradual return to sport is encouraged
Frequently asked questions
Some tears can heal, especially if they occur in the outer vascular zone. Many degenerative tears improve with physiotherapy.
No—most do not. Surgery is used when symptoms clearly persist and affect your daily life.
Often yes, if symptoms allow. Pain, swelling or locking means you should modify activity and seek specialist advice.
No—it is usually a day-case keyhole procedure with small incisions and quick recovery.
Large tears, untreated mechanical symptoms or removal of large portions of meniscus may increase the risk over time. Preserving the meniscus is always the priority.
Your Journey with Me
- Assessment: consultation, examination and imaging review
- Diagnosis: full explanation of the type of tear
- Treatment Plan: conservative first, surgery only if required
- Procedure (if needed): arthroscopy tailored to your tear
- Rehabilitation: physiotherapy and personalised recovery plan
- Follow-up: ensuring you return safely to sport or normal activity
My priority is to help you recover quickly and protect the long-term health of your knee.


